My Evidence-Based Longevity Routine
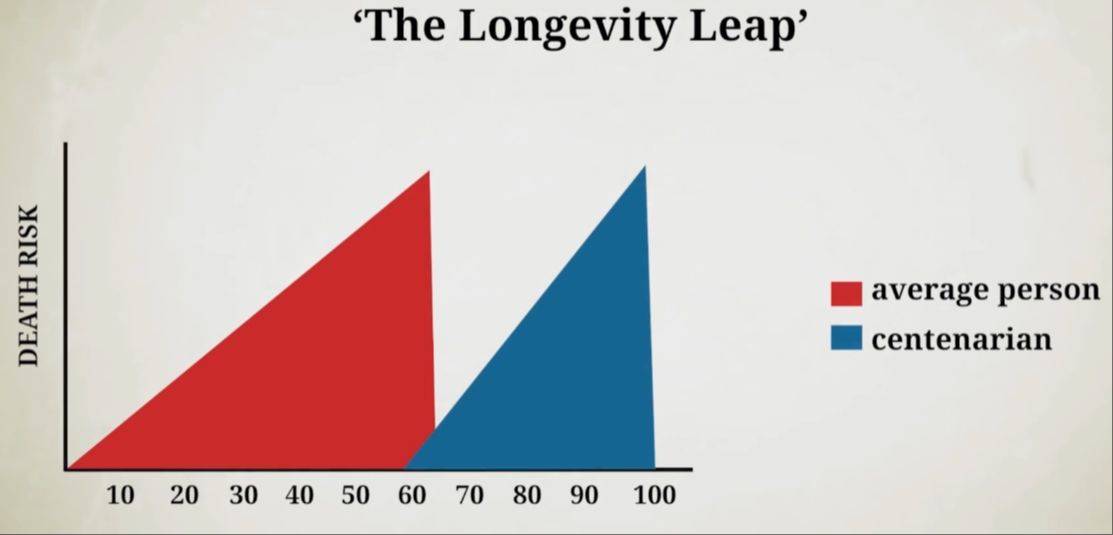
Longevity by definition is having a long life and staying alive. However, most people can’t achieve their longevity potential because they die of different chronic diseases like heart disease or cancer in their 60s and 70s. Coincidentally, the centenarians who live to 100 get the same diseases as everyone else but they get them a few decades later (R; R). So, living longer mostly comes down to avoiding the chronic diseases that would kill you prematurely. I call this The Longevity Leap.
Over the last 10 years, I’ve been working on my health and longevity in a preventive way – to make sure that I don’t die prematurely like my grandfather who passed away to colorectal cancer at the age of 36. That’s why in this video I’m going to outline my full evidence-based longevity routine. You will also hear commentary from 2 professors and researchers of aging Dr Matt Kaeberlein and Dr Michael Lustgarten.
My next book The Longevity Leap
Sign up for updates about my upcoming book The Longevity Leap: Unlock the Secrets to Slowing Down Aging and Adding Healthy Years to Your Life
Sign Up!
Body Composition
Let’s begin with my diet – more specifically one of the main goals of a healthy diet, which is maintaining good body composition. Obesity is one of the biggest risk factors for diabetes, cardiovascular disease, neurodegeneration, cancer, and kidney disease (R; R; R). An obese person can expect to live anywhere from 5-20 years less (R; R; R; R). Thus, to make the longevity leap and not die prematurely, you have to make sure you’re not overweight.
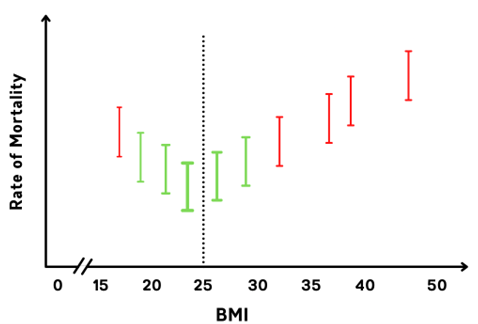
A 2009 analysis of prospective studies among 900,000 adults found that the lowest mortality is associated with a BMI of 22.5-25 (R). Based on this data, you would want to keep a BMI below 25 for the lowest risk of mortality.
However, BMI can be often misleading. For example, if you have even a little bit of muscle, your BMI might put you into the overweight category. There’s a lot of evidence suggesting that muscle mass and strength are inversely associated with all-cause mortality (R; R; R). Thus, having a bit more muscle mass may increase your BMI, but it might not increase your mortality risk because we know muscle is geroprotective.
Besides BMI, a more accurate measurement is your waist circumference. People with more weight around the midsection are at a higher risk of heart disease, diabetes, and premature death than those who carry it around their hips and thighs (R; R; R). You calculate your waist-to-hip ratio by taking your waist circumference and dividing it by your hip circumference (W/H). The lowest risk of heart disease is seen with a waist-to-hip ratio below 0.95 for men and 0.80 for women (R). With a waist-to-hip ratio above 1.0 for men and 0.86 for women, you would see the highest risk.
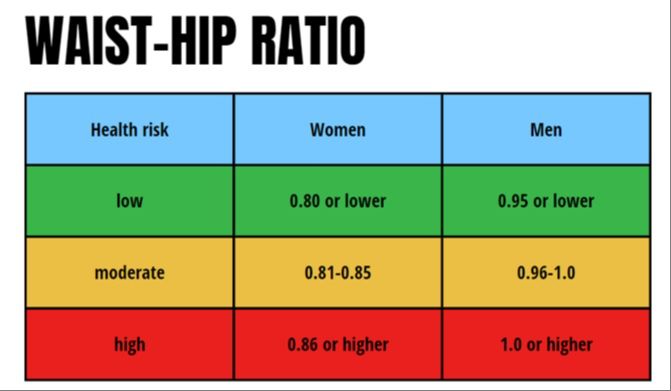
My goal is to keep my BMI around 25. Currently, it’s 25.5 but that’s because of muscle mass my body fat % is relatively low, around 10%. My visceral fat amount is virtually zero as my waist circumference is only 80 cm and my waist-to-hip ratio is less than 0.83. That puts me in the lowest risk category possible.
Calorie Restriction & Time-Restricted Eating
Next, we have to cover the most researched method of extending lifespan in virtually all animals, which is calorie restriction (R; R; R). Feeding fewer calories to different animals extends their lifespan up to 50% (R; R). The evidence of calorie restriction having longevity benefits in humans is obviously limited because it’s very difficult to conduct lifespan studies in humans. We do have a few randomized clinical trials on humans finding that calorie restriction improves multiple cardiometabolic risk factors even in young, non-obese adults (R; R; R).
I don’t think based on the evidence that you need to adhere to a specific calorie-restricted diet to live longer. You have to make sure that you don’t become overweight and obese. My own calorie intake falls somewhere between 2000-2500 on most days. That is what keeps my body fat percentage around 10% year-round while still being able to build muscle and strength.
One of the proposed ways to reap the benefits of calorie restriction without having to do it long-term is intermittent fasting, also known as time-restricted eating.
Research about time-restricted eating has found that it can improve markers of metabolic health, such as blood sugar, triglycerides, waist circumference, and cholesterol in obese as well as non-obese individuals (R; R; R; R). However, multiple randomized clinical trials from 2022 and 2023 have shown that time-restricted eating is not superior to regular calorie restriction (R; R; R). But there is evidence that eating most of your food during the daytime as opposed to at night is healthier (R; R; R).
Foods That Reduce Life Expectancy
Now, let’s move on with probably the most talked about part of longevity, which are the foods.
All successful diets that appear to be good for health have one thing in common – they minimize the consumption of ultra-processed food intake. Ultra-processed food intake is associated with an increased risk of cardiovascular events and all-cause mortality (R). It also increases the risk of dementia and Alzheimer's disease even after controlling for calorie intake (R). Based on the data, you could get away with 1-2 servings of ultra-processed food per day, but more than that is associated with an increased risk of dementia, CVD events, and all-cause mortality.
Foods That Increase Life Expectancy
If I were to describe my diet, then it would be a Mediterranean-style diet with a bit more protein and carbs. There have been many prospective studies finding an association between adherence to a Mediterranean Diet style of eating and reduced cardiovascular disease, cancer, and premature mortality (R; R; R; R; R).
What are some of the main components of the foods consumed on the Mediterranean diet? It’s polyphenols. A 2023 study from Spain found that a higher intake of polyphenols was associated with a 20% lower risk of all-cause mortality (R). This was mostly due to a 40% lower cardiovascular disease risk. Dozens of other cohort studies in different countries have found similar results (R; R; R). I have heart disease and cancer in my family, which is why I incorporate plenty of polyphenols into my diet.
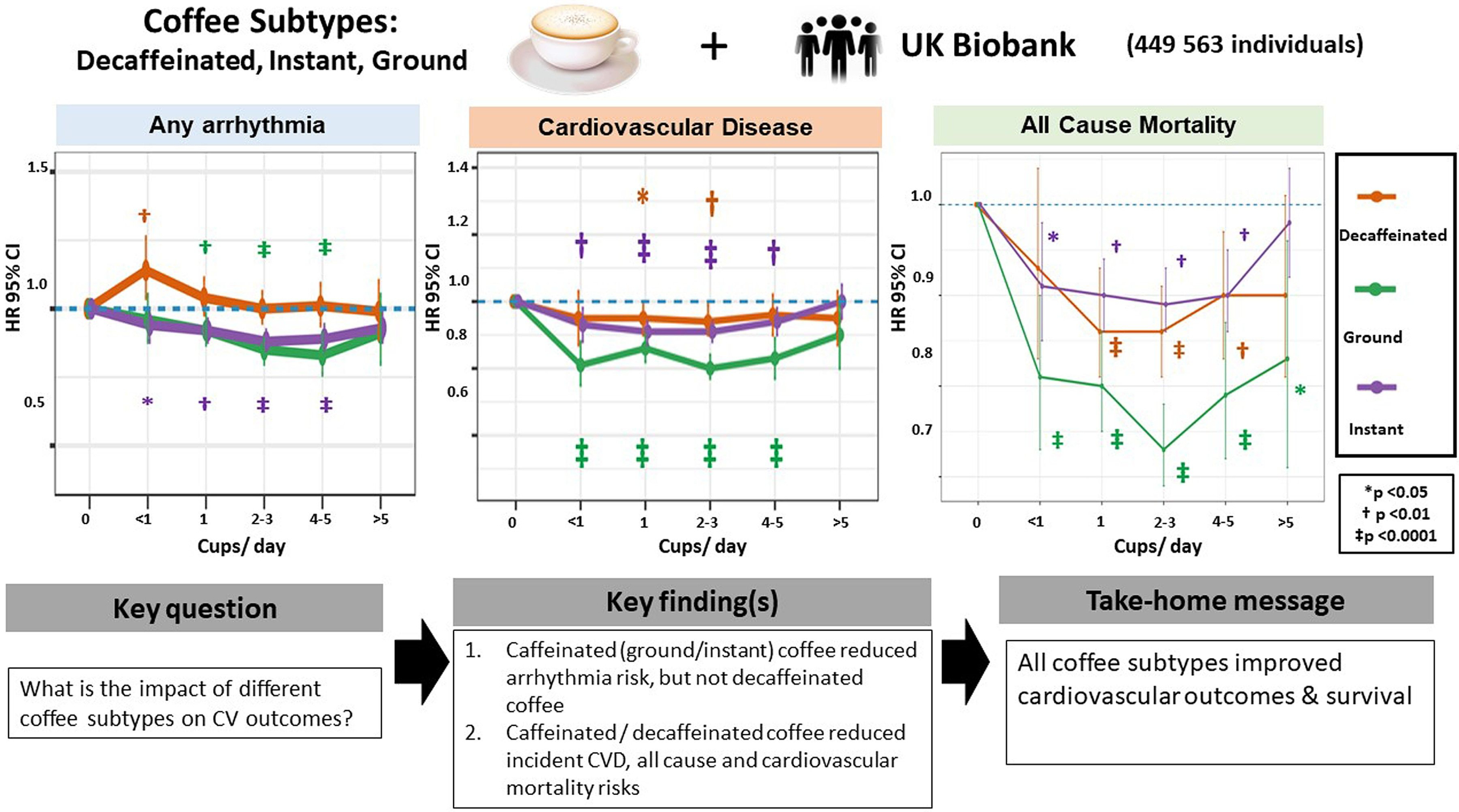
The most common source of polyphenols in the Western diet is coffee (R; R; R; R). Moderate coffee consumption is linked to a reduced risk of many diseases, such as colorectal cancer, liver cancer, heart disease, Parkinson’s, diabetes, and cardiovascular disease (R; R; R; R; R; R; R; R; R). A 2022 study found that decaf, ground, and even instant coffee all had benefits in reducing the risk of all-cause mortality and heart disease compared to non-drinkers (R). The lowest risk of death was -27% seen with 2-3 cups of ground coffee a day. I usually stick to 2 cups of coffee a day.
Another food group that reduces my risk of colorectal cancer and heart disease is fiber (R; R). People with a higher dietary fiber intake have been seen to have the lowest risk of atherosclerotic cardiovascular disease and colorectal cancer mortality (R; R). That’s why for my specific genetic history, a higher fiber diet is the best way to go.
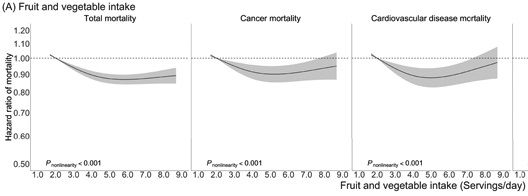
The RDA for total fiber intake for men is 38 grams/day and for women 25 grams/day (R). I personally get around 30-40 grams of fiber per day from various sources, preferably from high polyphenol foods, such as cruciferous vegetables, but also tubers like carrots. A 2021 meta-analysis saw that a higher fruit and vegetable intake was linked to a lower risk of all-cause mortality with the benefits plateauing at 5 servings of fruit and vegetables per day (R). I’m getting at least 3-4 servings of vegetables per day and 1-2 servings of fruit per day, usually in the form of an apple, a banana, and some berries.
How Much Protein Do I Eat
Another important topic regarding longevity foods is protein intake. Protein is controversial in the longevity space as many people suggest that you need to be eating a low-protein diet to live longer. However, most of the evidence of higher protein intake shortening lifespan is in animal models (R).
When it comes to humans, then a low protein intake is associated with an increased risk of mortality in the elderly (R). A 2023 study on protein intake in elderly people over the age of 85 found that a higher protein intake was linked to a lower risk of mortality (R).
The RDA of protein for an average person is currently at 0.36 g/lb/day or 0.8 g/kg/day. However, many experts and nutritionists consider this to be inadequate (R), especially for the aging population (R). For muscle and strength gain, the optimal amount of protein appears to be between 0.8 and 1.0 g/lb. or 1.6-2.2 g/kg of lean body mass (R). That’s why I get about 0.8 g/lb of protein per day. I weigh around 80 kg, so a daily intake of 150 grams of protein is the upper limit of what I would benefit from in terms of muscle growth. On most days, I try to stick between 130-150 grams.
An important and controversial point to discuss when we’re talking about protein is the differences between plant-based protein and animal-based protein.
Higher consumption of red meat is generally seen to be associated with heart disease, cancer, hypertension, and overall mortality (R; R; R; R). Epidemiological studies are notorious for being confounded by the ‘healthy user bias’ – that people who eat red meat also tend to exercise less and follow other unhealthy habits. However, most of these studies tend to adjust for these factors and still find the association with increased risk. What’s more, a 2022 Adventist Health Study found that animal-based foods were associated with an increased risk of mortality even after adjusting for ultra-processed food intake (R). Thus, there might be an independent risk with higher meat consumption, but it’s very difficult to test it in a randomized controlled trial.
I’m not a big meat eater – I might eat about 1 pound of meat per week in total. Based on the current evidence, it’s not fully clear how big of an impact meat has on longevity. I know a lot of people will get upset because of this – both the carnivores and the vegans. My modus operandi for my longevity is more on the side of caution. In my mind, it’s better to be cautious than completely reckless. Especially given the fact my bloodwork is already perfect right now, my physical performance is also high, and I haven’t seen benefits to eating more meat.
How Many Carbs Do I Eat
Next, let’s talk about fats and carbohydrates. This is another dividing line in online diet cults – are you low carb or high carb – and people are as fervous on this subject as they are with meat and protein intake.
In epidemiology, many studies find a U-shaped association between carbohydrate intake and all-cause mortality with increased mortality below 40% and above 55% of calories from carbohydrates (R; R; R). The obvious limitation to this is that it’s epidemiology.
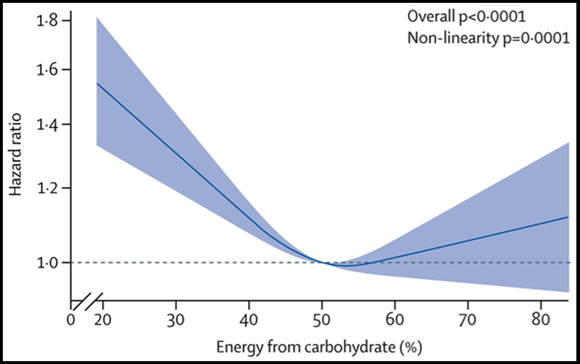
Diet quality matters here as well, as it’s been found that both unhealthy low-fat and low-carb diets increase mortality, whereas healthy low-carb and low-fat diets don’t (R; R). A higher fiber-to-carbohydrate ratio has also been seen to be associated with up to 20% lower risk of mortality (R). Eating more refined grains and refined sugars is linked to increased chronic diseases and mortality (R; R; R; R). Thus, it’s better to get more of your carbohydrates from fibrous vegetables, instead of refined carbohydrates. My main carbohydrate source, besides vegetables and fruit, is potatoes, but I sometimes also eat whole grains.
Based on the data, then the lowest mortality risk is around 40-55% of total calories as carbohydrates, which is where my carbohydrate intake generally falls into. I have no issues with my bloodwork, but I believe everyone should adjust their carbohydrate and fat intake based on what their bloodwork says. Only people with diabetes might benefit from carbohydrate restriction.
How Much Fat Do I Eat
I will briefly mention the different types of fats because they are quite relevant to longevity and disease risk.
In general, higher intakes of unsaturated fats, such as monounsaturated fatty acids (MUFAs) and polyunsaturated fatty acids (PUFAs), are linked to a lower risk of all-cause mortality (R). Trans fats have the highest association with mortality and saturated fats have a weaker link.
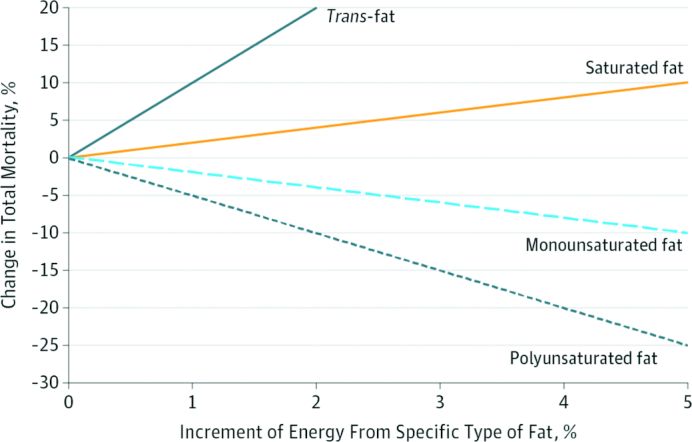
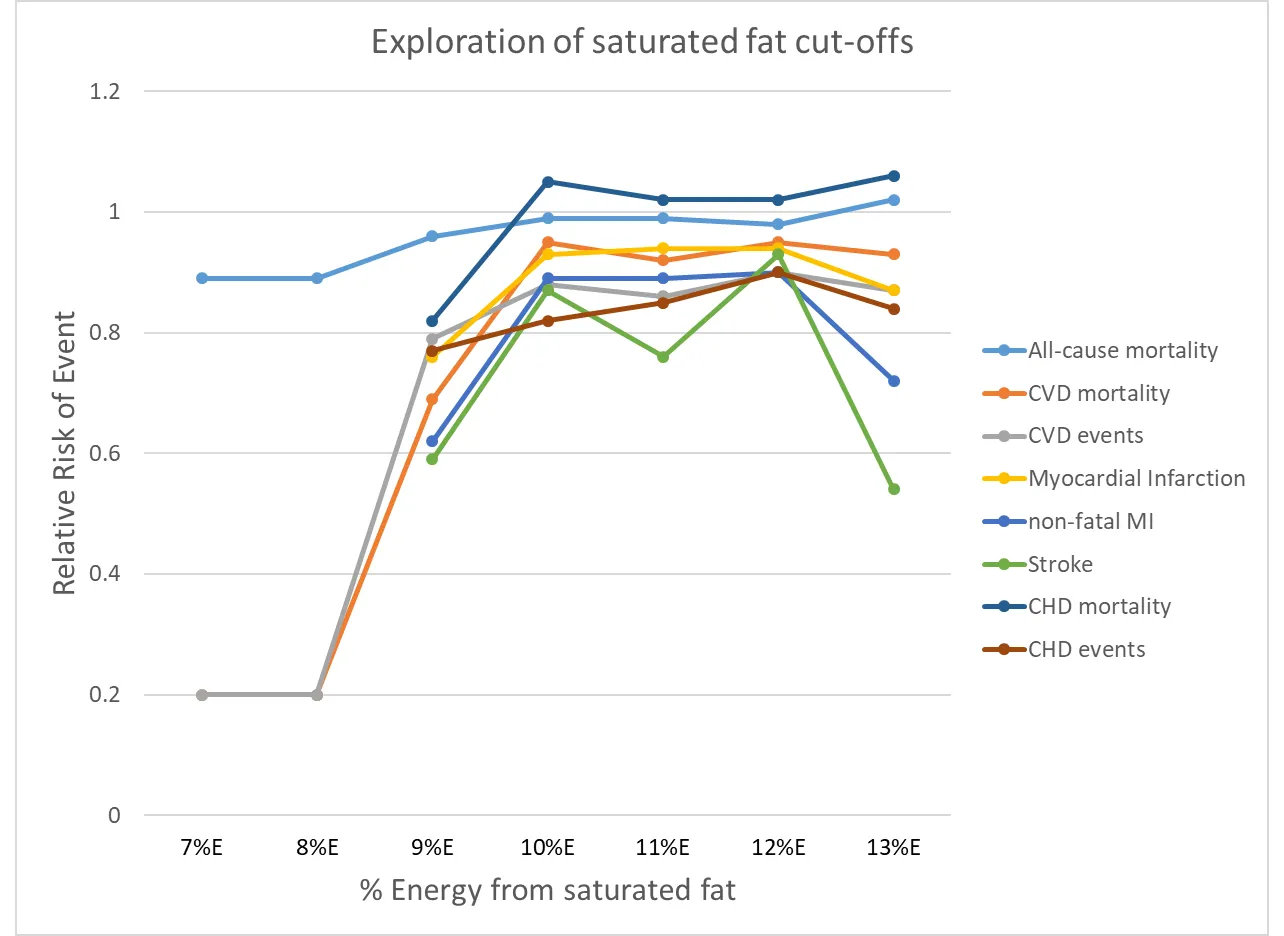
Many meta-analyses done in 2017, 2018, and 2020 involving over 1 million people suggest that saturated fat intake is associated with increased mortality and polyunsaturated fat intake is linked to decreased risk (R; R; R; R). A 2020 large Cochrane meta-analysis of 15 randomized controlled trials, which is one of the landmark analyses of saturated fat intake and CVD, found that the effect of saturated fat on cardiovascular disease follows an S-shaped association (R). Based on their results, the risk of CVD events and mortality starts to increase after 8% of total energy intake from saturated fat and the risk stays relatively the same from 9-13%. A 2020 UK Biobank study found that all-cause mortality started to increase after 10% of total calories came from saturated fat (R). Thus, a saturated fat intake that comprises less than 10% of your total calories appears to be most optimal for reducing the risk of CVD and all-cause mortality as also supported by a 2021 review (R).
However, the source of saturated fat plays a big role in risk. Dairy fat doesn’t appear to be associated with an increased risk of heart disease (R; R). At worst, it’s considered to be neutral and at best slightly positive (R). Chocolate also contains saturated fat, but moderate cocoa and dark chocolate consumption is associated with a reduced risk of CVD (R). However, these benefits of chocolate are mostly thought to be mediated by the flavonoids and polyphenols in unprocessed chocolate, and the stearic acid in chocolate is thought to be neutral (R; R). Thus, there might be benefits to small amounts of dark chocolate consumption thanks to its polyphenol and flavonoid content (R).
What’s most important is what you compare saturated fats to. If you replace saturated fat with refined carbs or trans fats, then the risk of CVD and mortality might be greater. But when you replace saturated fat with PUFAs or MUFAs or whole food high-quality carbohydrates, then the totality of evidence suggests a slight reduction in relative risk (R; R). Thus, it’s not that saturated fat inherently is that bad, it's just that other fats – PUFAs and MUFAs – and whole-food carbohydrates are better.
Overall, my philosophy about saturated fat is the same with meat – I try to minimize risk while maximizing reward. That’s why I’m getting less than 10% of my calories from saturated fat, primarily from dairy, dark chocolate, eggs, and meat. PUFAs and MUFAs I get mostly from olive oil and fish. There is a strong link between fish consumption and reduced risk of cardiovascular disease, neurodegeneration, and immunosenescence (R; R; R). People with the highest blood levels of EPA and DHA have been seen to have a lower risk of death from heart disease and Alzheimer’s (R; R). The recommended adequate intake of omega-3s is 1.1 g/day for females and 1.6 g/day for males (R). However, eating fish twice a week provides an average of only 300-450 mg/day. That’s not enough to meet the optimal amount. A combined intake of EPA and DHA between 1.75-2.5 grams/day has been found to be enough to reach omega-3 levels that are associated with reduced risk of CVD and death (R). That’s why I eat fish around 3-4 times a week and I take 1.5-3 grams of an omega-3 supplement every day. My total fat intake for the day is around 25-30%, which is more than enough. What I’m focusing more on is my bloodwork.
My Longevity Workout Routine
Next, let’s cover one of the most important factors of longevity, which is physical activity and exercise. Any form of exercise is generally beneficial to you. However, the main forms of exercise are generally categorized into cardiorespiratory fitness and strength training.
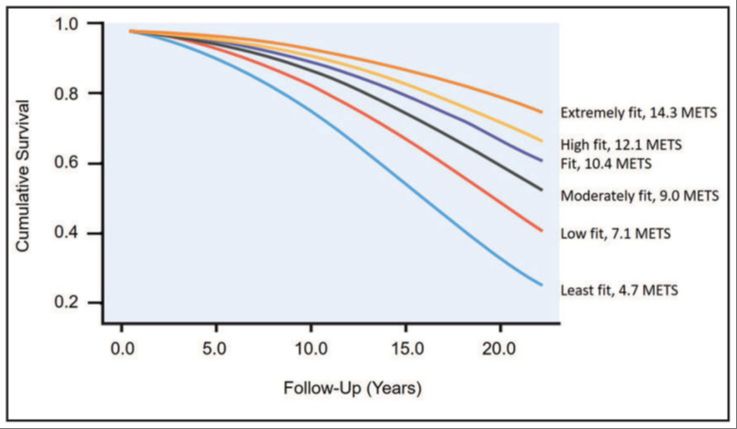
Cardiorespiratory fitness is inversely associated with long-term mortality with no observed upper limit of benefit (R; R). Compared to those with the lowest cardiorespiratory fitness, those with the highest cardiorespiratory fitness have been seen to have a 4-fold lower risk of mortality (R). Smoking typically increases your mortality risk by 2-3 times. Meaning, that being unfit is pretty much as bad as smoking.
The lowest mortality risk has been observed at a VO2 max of about 49-50 mL/kg/min (R). I have measured my VO2 max, and I got a score of 53, which puts me in the lowest risk category. You can increase your VO2 max with regular slow steady state cardio also called zone 2 training or with high-intensity interval training. The most optimal way is to obviously do both.
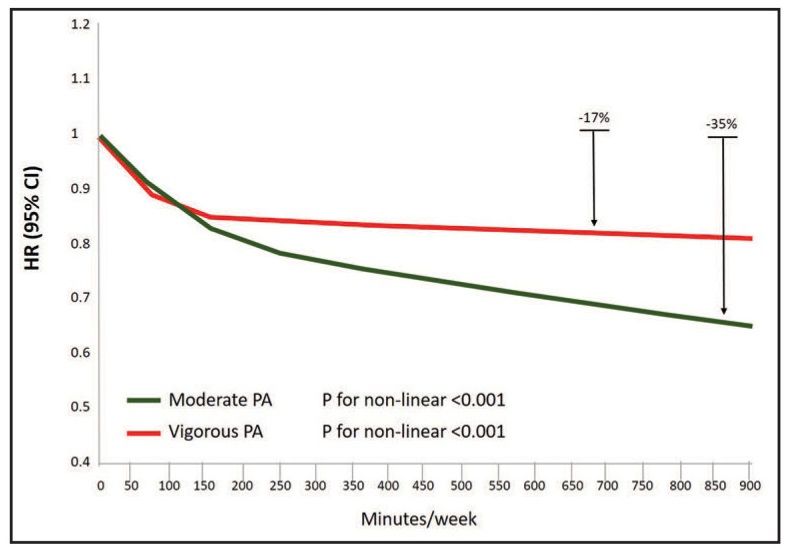
I do 1 interval workout per week and 2-3 zone 2 workouts per week because it’s associated with lower mortality risk in research. A 2023 systematic review found that the more moderate physical activity the lower your all-cause mortality risk (R). It even outperformed vigorous activity at high levels (-17% vs -35%). Thus, you don't get progressively more benefits the more vigorous exercise you do - you hit a plateau after 200 minutes/week. However, you do keep getting benefits the more moderate exercise you do (800 min/week is better than 200 min/week).
Next, Let’s Cover Strength
As we talked about earlier, muscle mass and strength are linked to reduced mortality (R; R; R). However, when comparing muscle mass and strength, a 2014 study found that those with low muscle mass alone saw a 23% increased risk of mortality (R). However, the individuals with low muscle strength were at a 98% higher risk irrespective of their muscle mass. Thus, having low muscle strength was linked to up to a 4 times greater risk of mortality than having low muscle mass alone. Both are obviously important, but muscle strength is a better indicator of overall health. That’s why I’m much more focused on muscle strength and quality of muscle.
How do you build muscle and strength? The best way to do so is with resistance training. You can do calisthenics, powerlifting, bodybuilding, CrossFit, etc. However, the main tenet and requirement is progressive overload, which basically describes getting stronger over time (R; R).
I’ve been doing resistance training for over 10 years, and I think it has had one of the most transformative impacts on my health. However, there have been several meta-analyses over the past few years that hint at how too much resistance training might increase your risk of mortality.
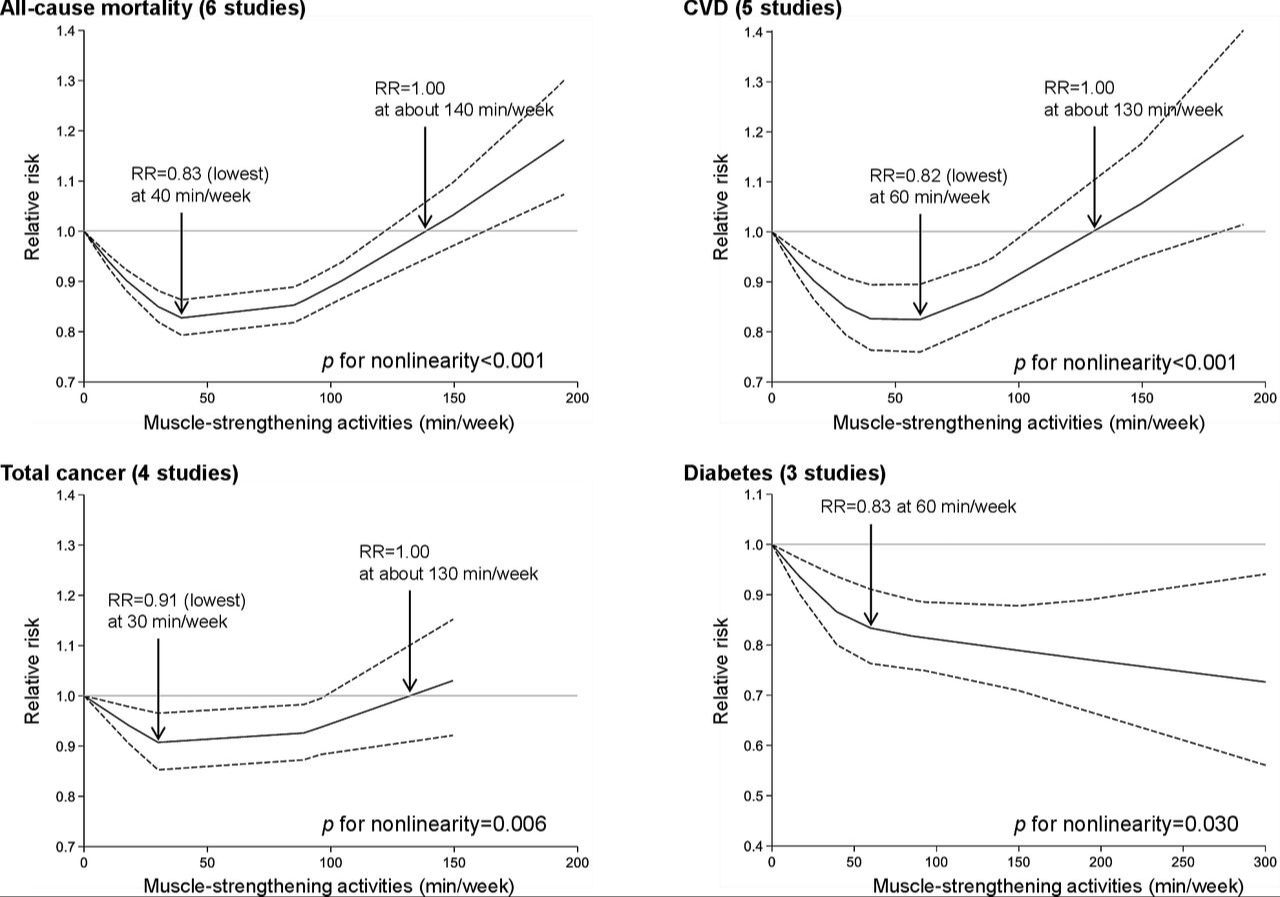
A 2022 systematic review and meta-analysis found that muscle-strengthening activities with resistance training were associated with a 10-17% lower risk of all-cause mortality, cardiovascular disease, cancer, and diabetes (R). The maximum risk reduction was observed at a dose of 30-60 minutes per week. However, after 60 minutes per week, the benefits started to diminish and beyond 140 minutes per week, resistance training was associated with an increased risk of mortality. Another 2022 systematic review and meta-analysis of 10 studies discovered similar results (R).
What’s the reason for this effect is not well understood. It’s thought it might have to do with increased arterial stiffness and chronic inflammation from too much training (R). Whether or not it’s true is still to be confirmed by randomized controlled trials. Based on the studies, if you're already lifting weights 3 times a week, which would give you around 100-140 minutes per week, then you won't gain any extra health benefits by adding an additional lifting workout. It might start to provide diminishing returns. After 3 lifting workouts per week, you would gain more benefits by adding more cardio instead.
The final component of exercise that I’m going to cover is walking.
A higher daily step count is linearly associated with lower all-cause mortality and cardiovascular disease (R; R). A 2020 JAMA study showed that walking 12,000 steps per day was associated with a 65% lower risk of mortality compared to taking 4000 steps per day (R). There were no significant observed benefits beyond 12,000 steps.
Overall, it’s recommended to get at least 8-10,000 steps a day. I personally try to aim for at least 10-12,000 steps a day.
My Supplementation Routine
This is probably the most asked about topic of this video, which is supplementation. For the sake of this video, I’m going to mention a few of the supplements that do actually work and have reliable data supporting their benefits on either healthspan or aging in humans. You can check out my other video about my full supplement stack.
GlyNAC
The first supplement I’m going to start with is probably the most evidence-based over-the-counter longevity supplement out there. It’s called GlyNAC or just glycine and NAC.
Both glycine and NAC help to increase the body’s glutathione levels (R; R). With age, your glutathione levels decrease, which results in oxidative stress, inflammation, and other age-related conditions (R; R). A 2023 randomized clinical trial found that supplementing GlyNAC for 16 weeks in older adults improved glutathione deficiency, oxidative stress, mitochondrial dysfunction, inflammation, physical function, and 7 hallmarks of aging (R). A 2021 review outlined studies finding that GlyNAC supplementation provides the same benefits but also improves insulin resistance, cognitive decline, body composition, and muscle strength in older people (R).
Whether or not GlyNAC has any effects in younger adults without comorbidities is not clear and the effects would be probably not that significant. That’s why I’m not taking the GlyNAC combo every day but I will certainly start doing it in my 40s. Right now, I’m taking GlyNAC only a few times a week when I want to strengthen my immune system or fix the oxidative stress from circadian rhythm mismatch or something like that.
If you want to get GlyNAC, then I recommend the product by DoNotAge. Use code SIIM for 10% discount.
Glycine
However, I take glycine alone every day in quite large amounts.
One of the biggest reasons I take glycine besides boosting glutathione is collagen. There are many human trials showing that collagen peptides improve skin health and reverse signs of skin aging (R; R; R; R). Your skin collagen content starts decreasing in your 20s at a rate of about 10% per decade (R). By the age of 70, you could’ve lost up to 50% of your skin collagen content. Starting to take collagen in your 40s when you get the first permanent wrinkles is already too late – you need to be maintaining your skin collagen in your 20s already.
For optimal collagen turnover, it’s been found that you need at least 12 grams of glycine per day (R). However, your body needs 3 additional grams of glycine for other vital processes inside the body. That increases the minimum glycine demand to 15 grams per day to cover the optimal collagen turnover of 12 grams and 3 grams of glutathione synthesis. If you’re eating an average diet, then you’ll still need at least 10 grams of extra glycine per day.

So, here’s what I do to get at least 12 grams of glycine per day.
- I take a collagen peptide supplement. If you take 10 grams of collagen peptides, then you’re going to get 3 grams of glycine from that. The brand of collagen I’m using Noord Code actually has an extra 5 grams of added glycine. So, I’m getting 8 grams of glycine per scoop of their complete collagen. They also have added eggshell membrane, which has been shown to improve joint health, and vitamin C, which is essential for initiating collagen synthesis. You can get the Noord Code Complete Collagen from https://www.noordcode.com and use the code SIIM10 for a 10% discount
- I also eat glycine-rich foods: fish with the skin, chicken skin, gelatin, etc. From dietary sources, I might be getting 2-3 grams of glycine.
- Lastly, I might take 5-6 grams of glycine as a powder, and I add it to my tea or yogurt because it tastes sweet.
In total, I’ll be getting at least 15-18 grams of glycine in total per day
Creatine
Moving on with creatine. There’s a lot of research about how creatine increases maximal strength, power, near-maximum intensity exercise, and lean body mass, and even reduces the incidence of injuries during training (R; R; R).
But creatine also has many longevity-boosting effects. It slows down age-related muscle loss and other disorders, such as neurodegeneration, memory impairment, and stroke (R). Creatine has been shown to slow down the progression of Parkinson’s in humans (R). Thus, creatine not only improves aspects of your physical health, but it also has benefits for your cognitive aging and brain health (R).
Dietary sources of creatine are red meat and fish, but you would have to consume a very large amount to reach the efficacious dose of 3-5 grams/day. Thus, supplementation with creatine is the easiest and most effective way to get an effect.
Metformin
There are also some very popular pharmaceuticals claimed to have longevity benefits. I’ll cover two of the most known ones.
Metformin is a potent anti-diabetic drug that lowers blood sugar and insulin. In diabetics, metformin does reduce the risk of cardiovascular and all-cause mortality (R). So, if you have diabetes, then metformin can be lifesaving, but many longevity enthusiasts are taking metformin off-label as well. Is it worth it?
In 2014 there was a study that suggested that diabetics taking metformin could live 15% longer than non-diabetics not taking metformin (R). However, the problem is that it was an observational study and they didn't control for any other variables. A recent 2022 reassessment of that 2014 study found that in case control pairs using metformin was found to be associated with increased mortality no matter the dose (R).
The danger of taking metformin as a non-diabetic for recreational use and for longevity purposes is that it has many negative effects on your fitness. Metformin reduces VO2 max (R) and may blunt muscle hypertrophy in response to resistance training (R). As we’ve already covered, having a higher VO2 max, muscle mass, and strength are one of the best predictors of longevity and reduced mortality.
If you don’t have diabetes and you’re taking metformin recreationally in hopes of extending your lifespan, then you might be doing yourself a disservice. Especially if you don’t have any poor glycemic control or insulin resistance.
Rapamycin
Rapamycin also known as Sirolimus is a pharmaceutical drug that’s most used in kidney transplant patients to prevent organ rejection (R). However, because it also inhibits a major growth pathway in the body called mTOR (R), many longevity enthusiasts are taking rapamycin in hopes of slowing down aging and living longer (R).
Rapamycin inhibits mTORC1, which has been seen to extend lifespan in animal studies by up to 60% (R; R; R)! There are no clinical trials on rapamycin’s effects on human longevity yet, but in clinical trials, rapamycin has been seen to be safe and well-tolerated (R; R).
In organ transplant patients, rapamycin has been seen to reduce the incidence of various cancers as well thanks to inhibiting mTOR (R; R; R; R). This is very interesting to me not only because of the longevity benefits but because of my grandfather. There are no human clinical trials on rapamycin and colorectal cancer specifically. However, rapamycin analogs are FDA-approved for various cancers (R) and they have been found to improve survival among cancer patients (R; R; R; R). So, if I ever get cancer, then I would consult with a medical professional first, but I would consider rapamycin in combination with other treatments.
A 2023 study by Matt Kaeberlein and colleagues evaluated the use of off-label rapamycin by 333 adults who were taking it for longevity purposes (R). Most of the people didn’t know if the drug was working or not, but they did self-report improvements in their health. However, the placebo effect can be quite strong in these kinds of people who are getting out of their own way to take a pharmaceutical drug off-label. Thus, there’s no way to know if it actually works in healthy people.
So, based on the current evidence, there’s no reason for me to take either rapamycin or metformin because at my age I have very little to gain even mechanistically. In fact, at my age, rapamycin and metformin could potentially have negative side effects.
If you want to learn more about Matt’s project and submit your own supplement for research, then head over to https://orabiomedical.com/
My Sleep Routine
Let’s move on with one of the most overlooked aspects of longevity, which is sleep.
First, how much sleep do we need? The recommended amount of sleep is 7-9 hours for adults (R).
A 2010 systemic review conducted at the University of Warwick saw that the risk of death was 12% higher for people who slept 6 hours or less (R). On average, I sleep about 7-8 hours per night and sometimes 9 hours if I need more recovery from exercise (R).
Here are some of the main things I do to sleep better.
- Consistent Bed Time and Wake Up Time –It improves sleep onset, overall sleep quality, and recovery (R). A consistent bedtime is also associated with better health and weight loss in young adult women (R). I usually go to bed at 9:30 PM and I’m asleep by 10 PM. In the morning, I wake up around 6-7 AM.
- Avoid Bright Lights at Night – Artificial blue light between the wavelength of 455-500 nM suppresses melatonin the main sleep hormone (R). Melatonin is not only important for sleep, but also for antioxidant defense, anti-aging, and managing inflammation (R). Suppression of melatonin at night is linked with obesity, metabolic syndrome, cardiovascular disease, depression, and cancer (R; R; R; R). To minimize the bright light exposure in the evening, I wear blue blocking glasses about 1 hour before bed. The brand of blue blockers I use to filter out the specific wavelengths of light that inhibit melatonin. You can check them out at https://boncharge.com/siimland and use the code SIIM for a 15% discount.
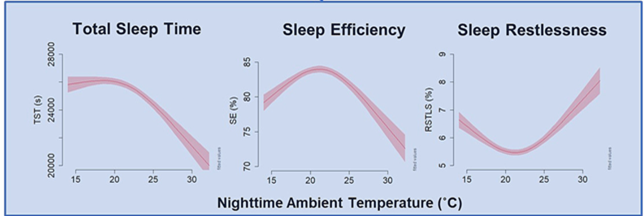
- Sleep in a Cooler Room - Sleeping at high temperatures decreases REM and deep sleep (R). People with difficulties staying asleep often have elevated core body temperature at night (R). According to the National Sleep Foundation, the best temperature for sleep is approximately 59–66.2°F (15–19°C) (R). However, a 2023 study on older adults saw the highest sleep efficiency at a temp between 20-25°C (R). Both high and low temp is harmful to sleep efficiency. At the end of the day, you have to find what works best for you.
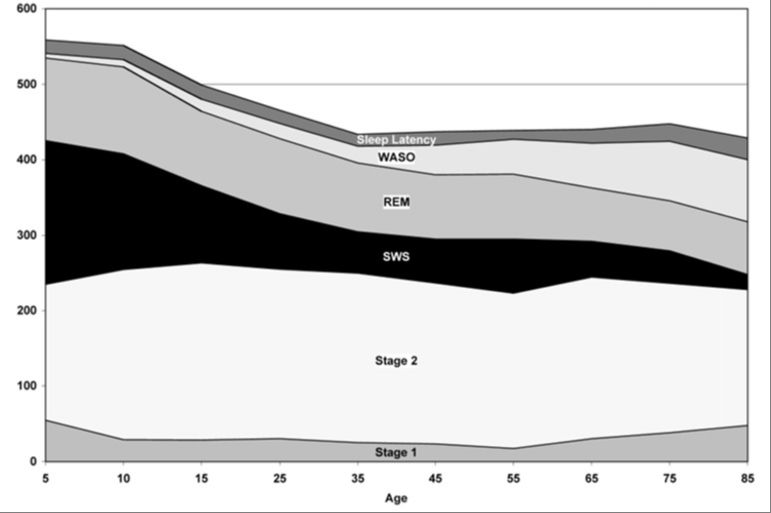
With age, you see a decrease in sleep quality and quantity, characterized by reduced sleep efficiency, increased fragmentation, more awakenings, and increased time it takes to fall asleep (R; R; R). More specifically, there’s a decrease in slow-wave sleep also called deep sleep and REM sleep (R), which are both critical stages of sleep for repairing the body and brain. Declining sleep quality accelerates the development of all the hallmarks of aging and biological aging (R).
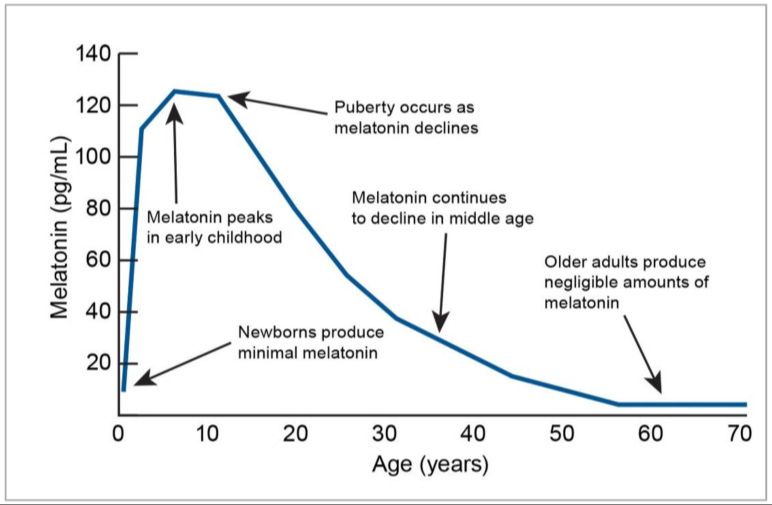
The biggest reason why your sleep deteriorates with age is damage to the circadian system (R; R). The master circadian clock inside the brain called the suprachiasmatic nucleus (SCN) becomes more susceptible to age-related impairment in the form of neuronal degeneration (R). As a result, your body starts producing a lot less melatonin with age. Older people produce significantly less melatonin than children and teenagers or even adults in their 20s and 30s (R; R). Because of decreased melatonin, seniors wake up more frequently, fall asleep slower, and spend less time in deep and REM sleep (R; R). This age-related decline in melatonin production is not a good thing and it does contribute to the acceleration of aging you see in your 50s and 60s. If we can mitigate it or postpone that decline, then we will not only improve our sleep quality but also extend healthspan.
One of my additional longevity strategies is microdosing melatonin just to fill the gap between how much our bodies make and what would be optimal. There’s evidence showing that melatonin supplementation before bed can help you to fall asleep faster and get more deep sleep but also increases total sleep duration and sleep quality (R; R; R; R; R). However, I’m more interested in the additional antioxidant and anti-inflammatory benefits of melatonin for cardio- and neuroprotection (R; R). Melatonin supplementation has been seen to improve risk factors of cardiometabolic health, such as lipids, blood sugar, blood pressure, and endothelial function (R; R; R; R).
The pineal gland makes around 0.1-0.9 mg of melatonin per day (R; R), depending on age and health status. Taking like 0.3 mg per night starting in your late 20s I think is a very viable and safe strategy for healthspan. There’s also no fear that it’s going to suppress natural melatonin production as doses up to 50 mg/day haven’t been shown to do so (R; R). However, melatonin at very large doses of 75 mg and above acts as a contraceptive (R). The brand of melatonin I take is Symphony Natural and they have the world’s first plant melatonin called Herbatonin made of phytoplankton. Herbatonin has been demonstrated to have 470% stronger antioxidant properties and 640% greater anti-inflammatory effect than synthetic melatonin (R). Herbatonin is my go-to melatonin for better sleep and the longevity benefits of melatonin. Melatonin is the most powerful anti-aging hormone your body has. To try out Herbatonin, head over to symphonynaturalhealth.com and use the code SIIM10 for a 10% discount. If you’re experiencing jet lag or chronic sleep deprivation, then the 3 mg dose of Herbatonin might work better.
My Sauna Routine
Another cornerstone part of my longevity routine is regular sauna use. I’m sure many people have heard that saunas can be beneficial for cardiovascular health and neurodegeneration. Indeed, taking the sauna >4x a week compared to 2-3x is associated with 63% lower risk of sudden cardiac death, 63% reduced heart disease mortality, 50% lower fatal cardiovascular disease, 48% lower fatal coronary heart disease, 46% lower risk of hypertension, and 40% reduced all-cause mortality (R; R). Sauna bathing is also associated with reduced dementia and neurodegeneration (R). Those using the sauna 4-7 times a week have a 66% lower risk of dementia and 65% lower risk of Alzheimer’s disease compared to doing so once a week (R). Those are quite insane numbers, especially given the fact that it’s compared to taking the sauna once a week. Imagine what would the risk reduction be compared to zero times a week. It could be even higher than that.

Based on the research I’ve just outlined, the optimal dose for taking a sauna is about 15-30 minute sessions at about 70°C to 100°C (156-212°F) about 2-4 times per week. Even once every 7 days will be better than nothing. I go to the sauna about 4 times per week for 15-20 minutes per session. That already gives me the maximum risk reduction and health benefits. There’s no need to do more than that but sometimes going to the sauna can also be a good way to reduce stress or make up for sleep deprivation. If the temperature is mild around 70°C, then I’ve never felt more stressed out or tired after the sauna. It actually makes me less stressed and more recovered.
Conclusion
So, here’s the framework for my evidence-based longevity routine through the Longevity Leap philosophy. My main goal at my age is to maintain my peak physical fitness, cognitive function, and overall health for as long as possible. What I’m doing right now could be completely different from what I’ll be doing at the age of 40, 50, or 80 but the main principles are going to be the same – stay fit and healthy. I highly encourage you to check out the blog post in the description that contains the audio transcript of this video as well as all the references for you to check out.
The Longevity Leap is going to be the title of my upcoming book. It covers all the information I talked about here and a lot more. You can sign up for updates about the book at www.thelongevityleap.com Everyone who signs up will also get access to the bonus material and a bonus chapter about my personal daily routine and supplementation once the book is finally released early 2024.
My next book The Longevity Leap
Sign up for updates about my upcoming book The Longevity Leap: Unlock the Secrets to Slowing Down Aging and Adding Healthy Years to Your Life
Sign Up!